The ‘Ten Commandments’ for the 2023 European Society of Cardiology guidelines for the management of endocarditis
24 April 2024
The ‘Ten Commandments’ for the 2023 European Society of Cardiology guidelines for the management of endocarditis
Prevention: Patient education plays a vital role in the prevention of IE. Patient groups can be identified as high-risk, intermediate-risk, or low-risk of developing IE. General preventative measures are recommended for intermediate-risk and high-risk patients, while antibiotic prophylaxis prior to dental procedures is recommended for the high-risk group only.
Endocarditis Team: The Endocarditis Team is essential for the management of IE patients. The Endocarditis Team consists of a minimum of a cardiologist and infectious disease specialist in referring centres, while many more disciplines are involved in heart valve centres including mandatory cardiac surgical capabilities. Regular communication between centres is recommended, and transfer of patients to a heart valve centre is indicated in patients who develop a complicated course.
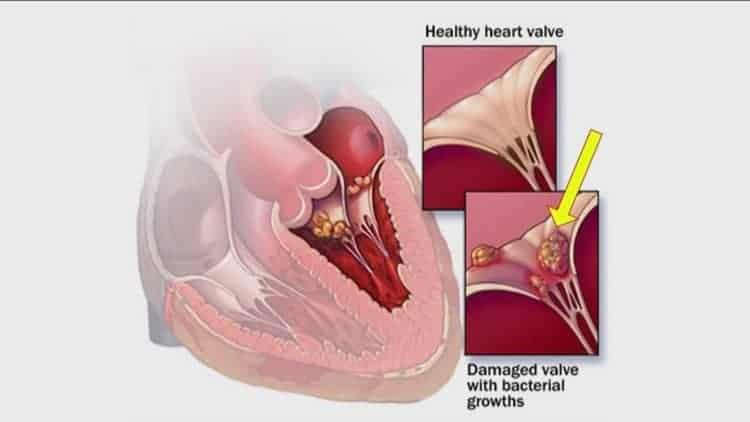
Diagnosis: Clinical, microbiological, and echocardiographic evidence remain the cornerstones of IE diagnosis. However, advanced cardiac imaging including cardiac CT, PET/CT, and WBC SPECT/CT are recommended in patients with possible IE and are now listed as major criteria in the 2023 ESC-modified IE diagnostic criteria if valvular or paravalvular involvement is confirmed. In addition, these techniques may confirm peripheral lesions as minor criteria.
Outpatient parenteral and partial oral antibiotic therapy: Select patients who have reached clinical stability after at least 10 days of appropriate intravenous antibiotic therapy or 1 week after corrective surgery should be switched to outpatient parenteral or partial oral antibiotic therapy. Repeat TOE is indicated to rule out disease progression before switching therapy.
Surgical indications and timing: Surgery is associated with improved survival, with the worst prognosis observed in patients with surgical indications that do not undergo surgery. The main surgical indications remain heart failure, uncontrolled infection, and embolism. Recommended timing is classified as emergency (<24 h), urgent (within 3–5 days), or non-urgent (within same hospitalization), depending on the indication for surgery.
Musculoskeletal IE complications: Magnetic resonance imaging or PET/CT is recommended in patients with suspected spondylodiscitis or vertebral osteomyelitis. Echocardiography is indicated in patients with spondylodiscitis/septic arthritis and positive blood cultures for typical IE organisms.
Neurologic IE complications: Timely mechanical thrombectomy may be considered in patients suffering embolic stroke. IE surgery should not be delayed in patients with ischaemic stroke, as well as those with haemorrhagic stroke and favourable brain bleed features.
Prosthetic valve and transcatheter valve IE: Prosthetic valve endocarditis (PVE) is associated with worse outcomes than native valve IE. Surgery is recommended for early PVE (within 6 months of valve surgery). Patients with transcatheter valve IE can be challenging to diagnose and manage, with surgery reserved for select patients.
CIED-associated IE: CIED-associated IE is associated with significant morbidity and mortality. Complete system removal is recommended in patients with definite CIED-associated IE and considered in patients with probable CIED-associated IE with persistent bacteraemia.
Right-sided IE: Right-sided IE is increasing in frequency due to increased CIED implantation rates as well as intravenous drug usage in certain regions. Surgery is indicated in select patient groups.