A. Left Ventricular Hypertrophy ECG Criteria
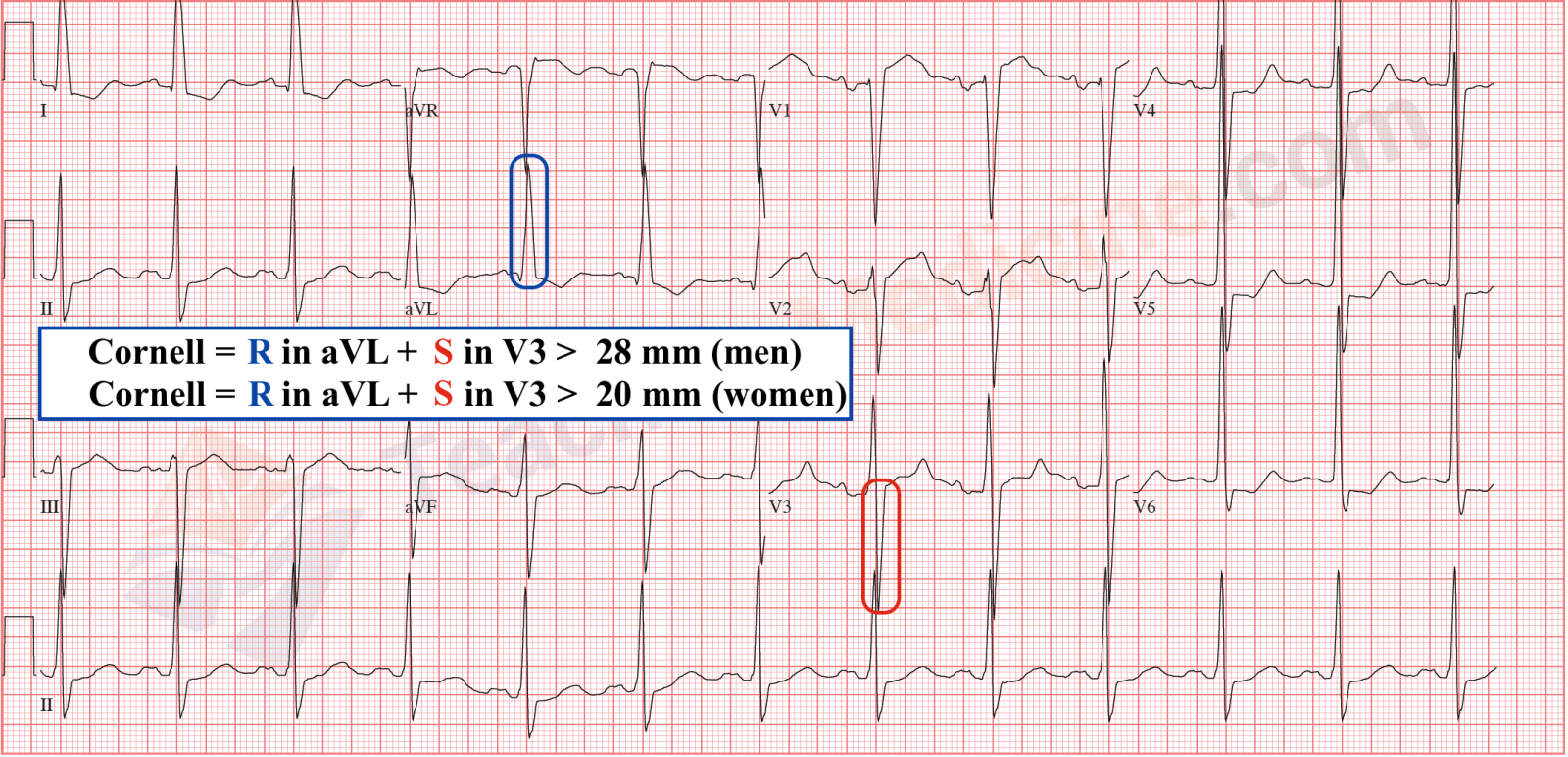
Cornell criteria: Add the R wave in aVL and the S wave in V3. If the sum is greater than 28 millimeters in males or greater than 20 mm in females, LVH is present. This criteria has the highest sensitivity in diagnosing LVH
Modified Cornell Criteria: Examine the R wave in aVL. If the R wave is greater than 12 mm in amplitude, LVH is present.
Sokolow-Lyon Criteria: Add the S wave in V1 plus the R wave in V5 or V6. If the sum is greater than 35 mm or R in aVL > 11 mm, LVH is present.


- Romhilt-Estes LVH Point Score System: If the score equals 4, LVH is present with 30% to 54% sensitivity. If the score is greater than 5, LVH is present with 83% to 97% specificity(highest specificity of all)
Amplitude of largest R or S in limb leads ≥ 20 mm = 3 points
Amplitude of S in V1 or V2 ≥ 30 mm = 3 points
Amplitude of R in V5 or V6 ≥ 30 mm = 3 points
ST and T wave changes opposite QRS without digoxin = 3 points
ST and T wave changes opposite QRS with digoxin = 1 point
Left Atrial Enlargement = 3 points
Left Axis Deviation = 2 points
QRS duration ≥ 90 ms = 1 point
Intrinsicoid deflection in V5 or V6 > 50 ms = 1 point

2. Total QRS voltage of all precordial leads >175 mm
3. R in V6 > = V5
4. Gertsch Index: S III + max(R+S) in any precordial lead > 3.0 mV. Valid even with LAFB
5. Lewis score: R I + S III > 17 mm
6. New Criteria (published in JACC in March 2017) – Peguero – Lo Presti Criteria
The deepest S wave plus the S wave in lead V4 ≥2.3 mV for women and ≥2.8 mV for men) is more accurate and as specific as standard ECG criteria.

7. Others are : Cornell voltage-duration measurement and cornell regression equation
Criteria for diagnosing LVH in presence of LBBB
- R in aVL >= 11mm
- Electrical axis >= 40(or SV2>=RV1)
- SV1 + R in V5 or V6 >= 40 mm
- SV2>= 30 mm and SV3 >= 25 mm

Criteria for diagnosing LVH in presence of RBBB
- Max R/S precordial lead with LAD > 29mm
- S V1 > 2mm
- R V5,V6 > 15 mm
- S III + max R/S precordial(with LAD) > 40 mm
- R I > 11mm
B. Right Ventricular Hypertrophy ECG Criteria
- R in V1 >= 0.7 mV
- qR in V1
- R/S in V1 > 1 with R> 0.5 mV
- R/S in V5 or V6 < 1
- S in V5 or V6 > 0.7 mV
- R in V5 or V6 >= 0.4 mV with S in V1 <= 0.2 mV
- Right axis deviation
- S1Q3 pattern
- S1S2S3 pattern
- P pulmonale
- In presence of RBBB, R’ > 15mm
- Cabrera Index > 0.5(R in V1/R in V1+ S in V1)
Sokolow Lyon criteria for RVH
- R in V1 + S in V5,V6 > 10.5 mm
- R in V1 > 7 mm
- R in aVR > 5 mm
- S in V1 < 2mm
Buttler-leggett formula for RVH
Anterior(R or R’ in V1 or V2) + Right(deepest S in I or V6) minus posterolateral(S in V1) > = 0.7 mV
RVH morphology
- RAD
- ST-T changes in precordial leads(strain pattern)
- Delayed onset of intrinsicoid deflection
- Precordial voltage changes
- Normal QRS duration
CHOU types of RVH
- Type A: typical RVH with tall R in V1 and prominent S in V5,V6
- Type B: Incomplete RBBB(ASD,RHD) with R in V1 >0.5mV with R/S > 1, normal QRS in V5,V6
- Type C:Chronic lung disease(rS in V1,V2 and RS in V5,V6), ECG changes due to RVH and anatomical shift of heart

C. Bi-Ventricular hypertrophy
- LAD with counterclockwise rotation in RVH
- Large equiphasic QRS in mid precordial leads > 60 mm(Katz-wachtel phenomena)
- Diagnostic voltage criteria for both ventricles
- Delayed intrinsicoid deflection over both ventricles
- Repolarisation changes over both
- LVH with RAD
- LVH with RAE
- Deep S in LVH
- LVH with clockwise rotation of precordial morphology

D. Right atrial enlargement
- Peaked P wave in lead II with amplitude > 2.5 mm(P pulmonale)
- Prominent initial positivity in lead V1 or V2 > 1.5mm
- Increased area under initial positive portion of P wave in lead V1 > 0.06 mm-sec
- Rightward shift of mean P wave axis more than 75 degrees
- qR pattern in right precordial leads (100 % specific)
- Low amplitude QRS complexes in lead V1(< 0.6mV) with threefold or greater increase in lead V2(90 % specific)
- Severe RAE—>prominent terminal negativity in lead V1(pseudo LAE sign)
- Early terminal negativity in lead V1(<0.03 s)
E. Left atrial enlargement
- Prolonged P wave duration of > 120 msec in lead II
- Prominent notching of P wave in lead II with interval of two notches >40 msec
- Ratio of P wave duration in lead II and duration of PR segment > 1.6(Macruz Index)
- Increased duration and depth of terminal negativity of P wave in lead V1 so that area subtended > 0.04 mm-sec(Morris Index)
- Leftward shift of mean P wave axis between – 30 and -45 degrees
- Positive P terminal force in aVL (PPTF-aVL) > 0.5 mm







