Current global guidelines recommend the use of steroidal mineralocorticoid receptor (MR) antagonists (MRAs) for patients with HF with reduced ejection fraction (HFrEF).
The European Society of Cardiology guidelines suggest considering steroidal MRAs in HF with mildly reduced ejection fraction (HFmrEF) but not in HFpEF. However, their use has been linked to increased risks of hyperkalaemia, acute kidney injury and gynaecomastia
Finerenone is a selective, non-steroidal MRA that was approved in 2021 by the Food and Drug Administration to reduce the risk of sustained estimated glomerular filtration rate (eGFR) decline, end-stage kidney disease, CV death, MI and hospitalisation for HF (HHF) in patients with CKD associated with T2D.
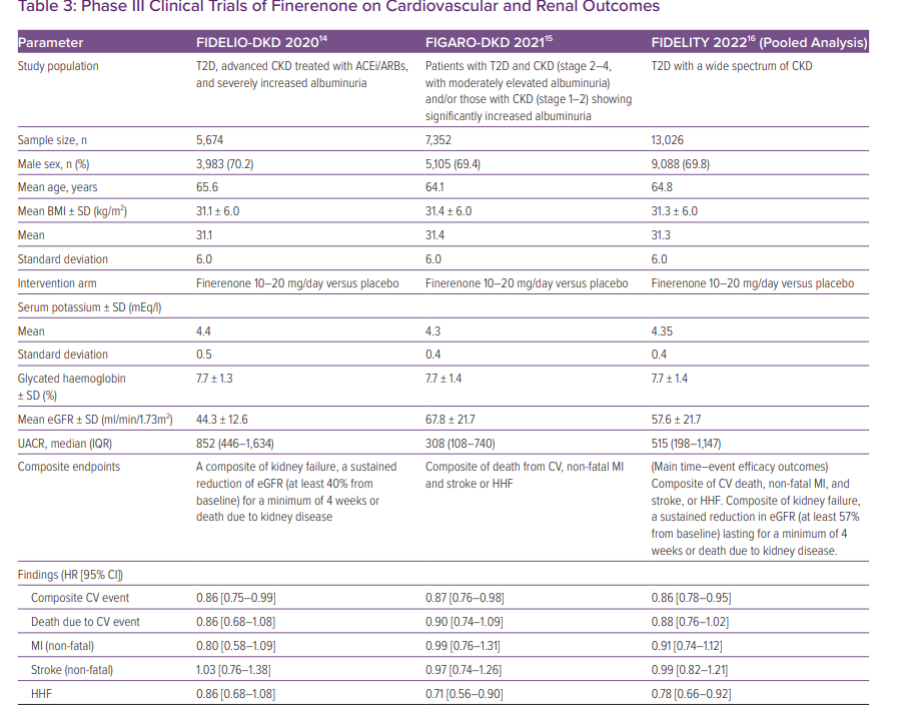
The initial approval of finerenone was based on the promising results of the pivotal Phase III FIDELIO-DKD trial, which indicated an 18% reduction in CKD progression events and a 14% reduction in CV events compared with placebo in patients with CKD and T2D
The FIGARO-DKD trial also highlighted that the CV benefits of finerenone were primarily driven by a 29% reduction in the risk of first HHF and a 32% reduction in the risk of new-onset HF in patients without a prior history of HF
A prespecified pooled analysis of both Phase III trials, FIDELITY, demonstrated that finerenone improved both CV and kidney outcomes across different stages of CKD severity
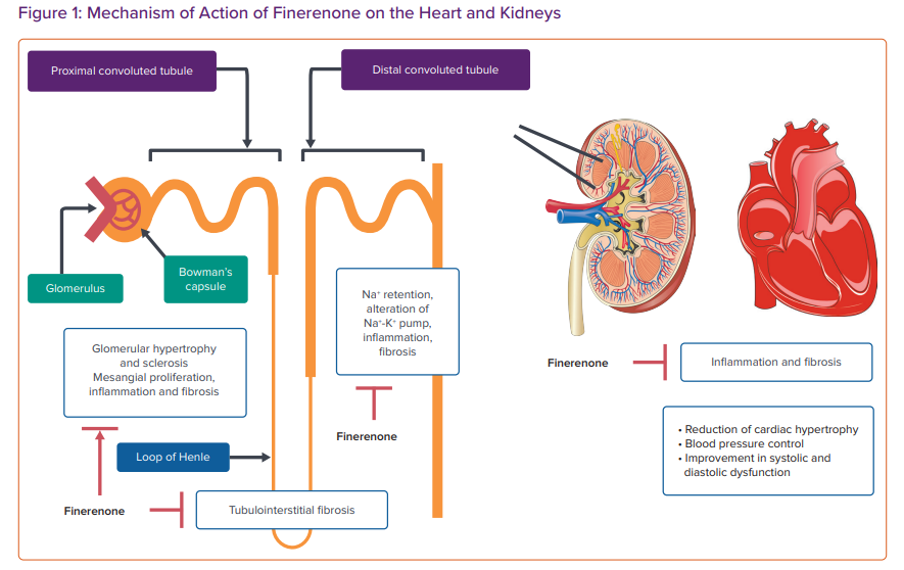
Finerenone, the first non-steroidal MRA, boasts remarkable potency and selectivity for the MR. It inhibits the binding of aldosterone and cortisol, thereby curtailing the recruitment of transcriptional cofactors essential for the expression of genes linked to hypertrophy, inflammation and fibrosis – traits typically associated with MR activation
Unlike traditional steroidal MRAs, finerenone exhibits a balanced distribution within both cardiac and renal tissues, has a shorter half-life, lacks active metabolites, and demonstrates superior MR selectivity compared with spironolactone, along with heightened receptor binding affinity relative to eplerenone
In the FIDELITY study, hyperkalemia was more common with finerenone than placebo, but incidence of clinically significant hyperkalemia-related events were low, leading to hyperkalaemia-related permanent discontinuation in only 1.7% of finerenone users versus 0.6% with placebo over a median 3-year follow-up. Hypokalemia was less frequent in finerenone-treated patients. Overall, finerenone improves cardiorenal outcomes in CKD and type 2 diabetes with a manageable hyperkalemia risk
Finerenone has shown promising potential in improving CV and renal outcomes in pivotal clinical trials involving patients with CKD and T2D (FIDELIO-DKD and FIGARO-DKD). FIDELIO-DKD and FIGARO-DKD also hint at a possible beneficial impact of finerenone on HFpEF. Finerenone demonstrated a significant reduction in the composite CV outcome, irrespective of HF.
Its higher selectivity and balanced tissue distribution between the heart and kidneys offer advantages over traditional steroidal MRAs, such as spironolactone and eplerenone, with fewer risks of hyperkalaemia and kidney function deterioration. The FINEARTS-HF trial found that finerenone significantly reduced the risk of worsening HF events or CV death in patients with HFmrEF or HFpEF.
Ongoing and upcoming large-scale clinical trials, including REDEFINE-HF, FINALITY-HF and CONFIRMATION-HF, aim to further elucidate the efficacy and safety of finerenone in a broad spectrum of HF populations, including those with HFmrEF and HFpEF.