The following are key points to remember from a state-of-the-art review on mavacamten, a first-in-class myosin inhibitor for obstructive hypertrophic cardiomyopathy (HCM):
HCM is caused by cardiac sarcomere dysfunction causing excess myosin-actin cross-bridging and increased calcium sensitivity.
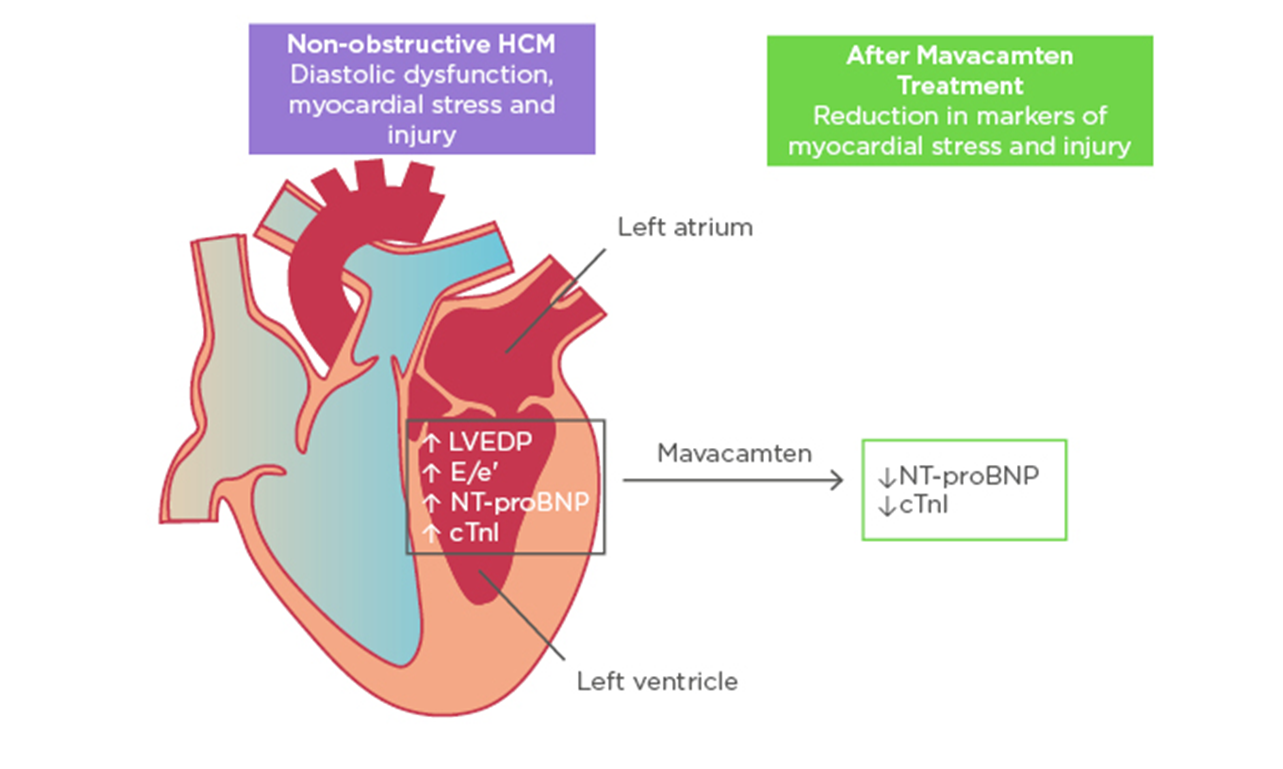
Mavacamten is a reversible myosin inhibitor that targets the core pathophysiological mechanism of HCM. It decreases the number of myosin heads that can interact with actin actively. It therefore reduces sarcomeric hyperactivity, reducing left ventricular outflow tract (LVOT) obstruction and decreasing LV filling pressures.
Mavacamten is extensively metabolized by CYP2C19 and CYP3A4 and has a high propensity for drug interactions. It has a long half-life of 6-23 days.
A phase 2 trial for mavacamten showed a dose-dependent benefit with reduction in LVOT obstruction, and improvement in New York Heart Association (NYHA) class and quality of life. LV ejection fraction (LVEF) remained over 50% in all patients.
EXPLORER-HCM was subsequently conducted as a phase 3 trial and to date is the largest placebo-controlled trial in obstructive HCM with a myosin inhibitor. Mavacamten was associated with an improvement in exercise capacity and symptom burden with improvement in Valsalva gradients, health status, and B-type natriuretic peptide (BNP) levels. Serious adverse event rates were comparable in the placebo and mavacamten groups (9% vs. 8% resp), and seven patients on mavacamten had a LVEF <50% that returned to baseline with drug discontinuation for the vast majority.
The impact of mavacamten on exercise capacity and NYHA class was greater in patients NOT on a beta-blocker. The efficacy of the drug in decreasing LVOT obstruction and reducing BNP levels was not altered by presence or absence of beta-blockade.
Imaging substudies demonstrated significant reductions in left atrial volume index, LV mass index, and LV wall thickness with mavacamten compared with placebo.
For the EXPLORER–long term extension (EXPLORER-LTE) study, mavacamten dose was adjusted based on echo measures of LVEF and Valsalva gradient as opposed to serum mavacamten levels used in the parent study. Benefits were again replicated in this study. Approximately 5% of patients discontinued mavacamten due to a drop in LVEF with >50% recovering function with drug discontinuation.
The VALOR-HCM trial randomized obstructive HCM patients with severe symptoms, referred for septal reduction therapy (SRT) to placebo versus mavacamten. At 16 weeks of treatment, significantly fewer patients in the mavacamten group needed SRT compared with placebo (77% vs. 18%). Benefits were sustained at 32-week follow-up.
Trial results extrapolate to a number needed to treat of 5.2 for mavacamten and suggest benefit with the drug in obstructive HCM patients with symptoms despite beta-blockers and/or calcium channel blockers.
The listed monthly price for the drug is $735. It is currently available in the United States through the REMS program for early detection of systolic dysfunction with close echo monitoring and to assess for drug interactions prior to each refill.