Multimodality Imaging for Pericardial Disease: Key Points
15 August 2024
Multimodality Imaging for Pericardial Disease: Key Points
The following are key points to remember from an international position statement on multimodality imaging for pericardial disease:
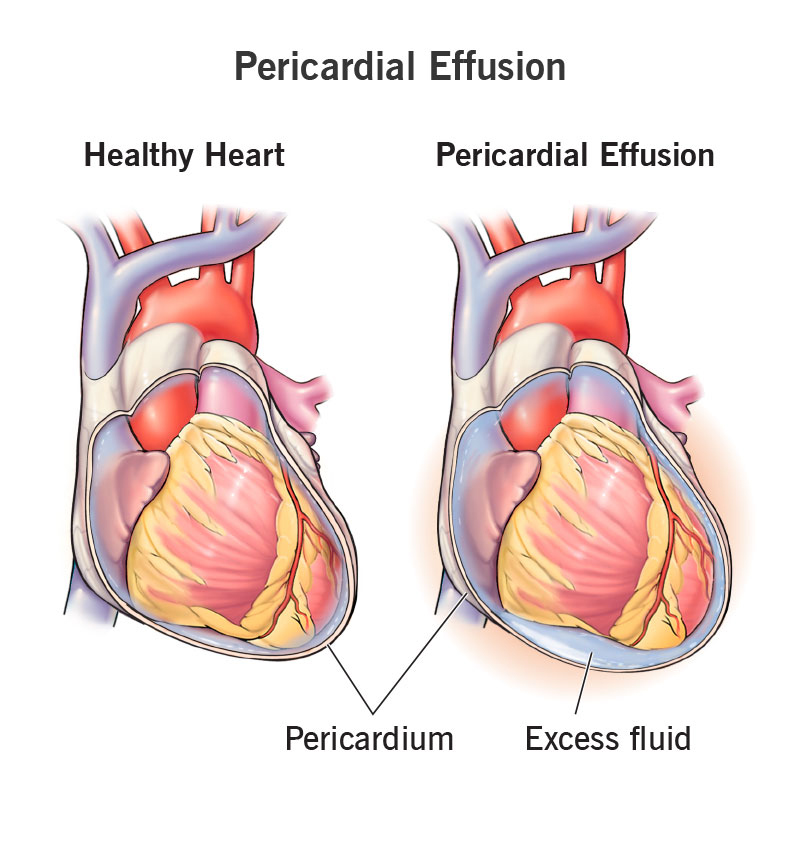
The spectrum of pericardial disorders encompasses pericardial inflammation, effusion, constriction, masses, and congenital anomalies. Pericardial diseases have gained renewed clinical interest leading to a new renaissance in the field.
There have been many recent advances in pericardial diseases in both multimodality cardiac imaging [MMI] of diagnoses such as recurrent, transient constrictive, and effusive-constrictive pericarditis, and targeted therapeutics especially anti-interleukin-1 (IL-1) agents that affect the inflammasome as part of autoinflammatory pathophysiology.
MMI now plays important roles in the diagnosis, prognostication, and surveillance of pericardial diseases. However, there remains a large educational gap for clinicians leading to variability in evaluation and management of these patients.
Recent clinical trials involving anti-IL-1 agents in recurrent pericarditis including anakinra (AIRTRIP trial), rilonacept (RHAPSODY trial), and goflikicept have demonstrated their efficacy. Biologic therapies including rilonacept necessitates imaging-guided therapy strategy to manage pericardial diseases.
This document represents an international position statement from world leaders in the pericardial field focusing on novel concepts, emphasizing the role of MMI as well as new therapeutics in pericardial diseases.
MMI plays a major role in assessing inflammation and edema (cardiac magnetic resonance [CMR]), pericardial effusion, and constrictive pericarditis physiology (transthoracic echocardiography [TTE]) in acute pericarditis to assess the hemodynamic consequences of constrictive pericarditis as in interventricular dependence (TTE and CMR) to location and degree of calcification (computed tomography [CT]).
TTE is usually first-line therapy due to its noninvasive nature, mobility, and low cost. CMR is becoming first-line in certain pericardial syndromes such as acute and recurrent pericarditis due to excellent imaging of inflammation, which can provide important information about prognosis and long-term outcome. CT scan excels with its ability to assess pericardial calcification and allows for preoperative planning in patients with previous open heart surgery.
Targeted therapies with anti-IL-1 agents with imaging-guided therapy using CMR now allows visualization of inflammation and edema and provides a roadmap to severity of therapy and prognosis.
In the noninflammatory phenotype, biologics are less likely to work and low-dose prednisone may empirically be started, although this strategy requires further research. Further studies are necessary to study the role of exercise and pericarditis and ability to exercise while on biologics.
Finally, tertiary pericardial centers of excellence have been initiated to provide expertise in diagnosis and management of these complex patients and to allow for the proper imaging-guided therapy with the newer anti-IL-1 agents.