Review and Treatment Options for the Tricuspid Valve: Key Points
4 May 2024
Review and Treatment Options for the Tricuspid Valve: Key Points
The following are key points to remember from an American Heart Association scientific statement, which reviews the pathology, imaging, and current treatment options for the tricuspid valve (TV):
TV disease is an often under-recognized clinical problem that is associated with significant morbidity and mortality.
Furthermore, patients will often present late in their disease course with severe right-sided heart failure, pulmonary hypertension, and life-limiting symptoms that have few durable treatment options.
Traditionally, the only treatment for TV disease has been medical therapy or valve surgery; however, there has been increasing interest and success with the use of transcatheter TV therapies over the past several years to treat patients with previously limited therapeutic options.
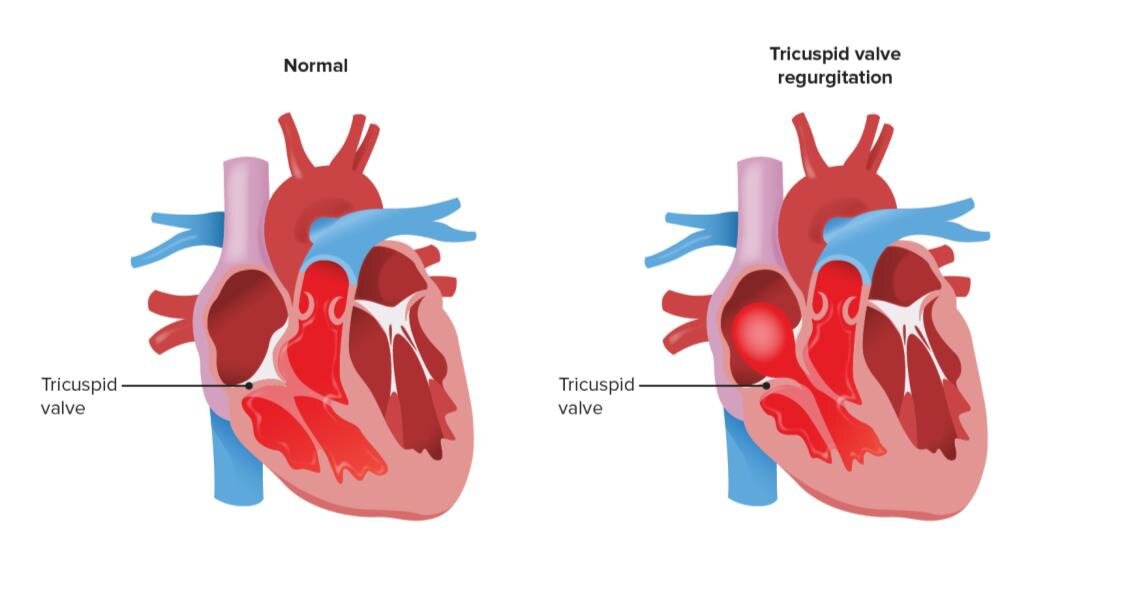
Of note, the TV is complex anatomically, lying adjacent to important anatomic structures such as the right coronary artery and the atrioventricular node, and is the passageway for permanent pacemaker leads into the right ventricle.
In addition, the mechanism of tricuspid pathology varies widely between patients, which can be due to primary, secondary, or a combination of causes, meaning that it is not possible for one device to be suitable for treatment of all cases of TV disease.
To best visualize the pathology, several modalities of advanced cardiac imaging are often required, including transthoracic echocardiography, transesophageal echocardiography, cardiac computed tomography, and cardiac magnetic resonance imaging. This detailed imaging provides important information for choosing the ideal transcatheter treatment options for patients with TV disease, taking into account the need for the lifetime management of the patient.
At present, there are no guidelines to determine whether an individual patient may be better suited for transcatheter TV repair or replacement, and although the understanding of the management of these patients is rapidly growing, the field is still evolving.
For patients with large annuli due to right ventricular failure, atrial fibrillation, or a combination, tricuspid transcatheter edge-to-edge repair (TEER) may be difficult, if not impossible, because of large coaptation gaps. These patients may be better suited for transcatheter TV replacement or transcatheter annuloplasty.
It is important to consider the lifetime management of patients with TV disease. When young patients present with severe tricuspid regurgitation, they will need a durable device and ideally the potential option of a second transcatheter device in the future should the first device deteriorate over time. For example, using an annuloplasty device first may leave open options for transcatheter TV replacement in the future, whereas a TEER device may not allow another device to be placed if it becomes necessary.
For elderly, frail patients, alleviating symptoms and improving their present quality of life may be the primary goal; therefore, long-term lifetime management may not be as applicable. As clinical studies continue, a greater understanding of device durability will allow clinicians to better advise patients about the long-term management of TV disease.