The ‘10 commandments’ for the 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes
27 February 2024
The ‘10 commandments’ for the 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes
Screening and cardiovascular risk assessment
Patients with type 2 diabetes (T2DM) exhibited an increased risk to develop cardiovascular disease (CVD) as well as chronic kidney disease (CKD), and the presence of these comorbidities in a given patient has a major impact on the prognosis and also on treatment strategies. Therefore, it is of utmost importance to identify patients with diabetes and CVD as well as patients with diabetes and CKD.
1. Given the high prevalence of undetected diabetes, it is recommended that all patients with CVD are screened for the presence of diabetes using fasting plasma glucose and HbA1C.
2. All patients with diabetes should be evaluated for the presence of CVD by assessing medical history and the presence of symptoms suggestive of atherosclerotic cardiovascular disease (ASCVD).
3. Systematic survey for heart failure (HF) symptoms and/or signs of HF is recommended at each clinical encounter in all patients with diabetes.
4. Patient with diabetes should be regularly screened for the presence of CKD by assessing estimated glomerular filtration rate defined by chronic kidney disease epidemiology/CKD epidemiology collaboration and urine albumin-to-creatinine ratio (UACR).
5. It is recommended to categorize CV risk in patients with T2DM based on the presence of ASCVD or severe target organ damage, or—in patients without ASCVD or severe target organ damage— based on the results of the dedicated T2DM CVD risk score, SCORE2-Diabetes.
Evidence-based, person-centred treatment strategies in patients with type 2 diabetes and cardiovascular disease
6. The use of glucose-lowering medications with proven benefit should be prioritized followed by agents with proven CV safety over agents without proven CV benefit or proven CV safety.
7. It is recommended to switch drugs from glucose-lowering medications without proven benefit or proven safety to drugs with proven benefit.
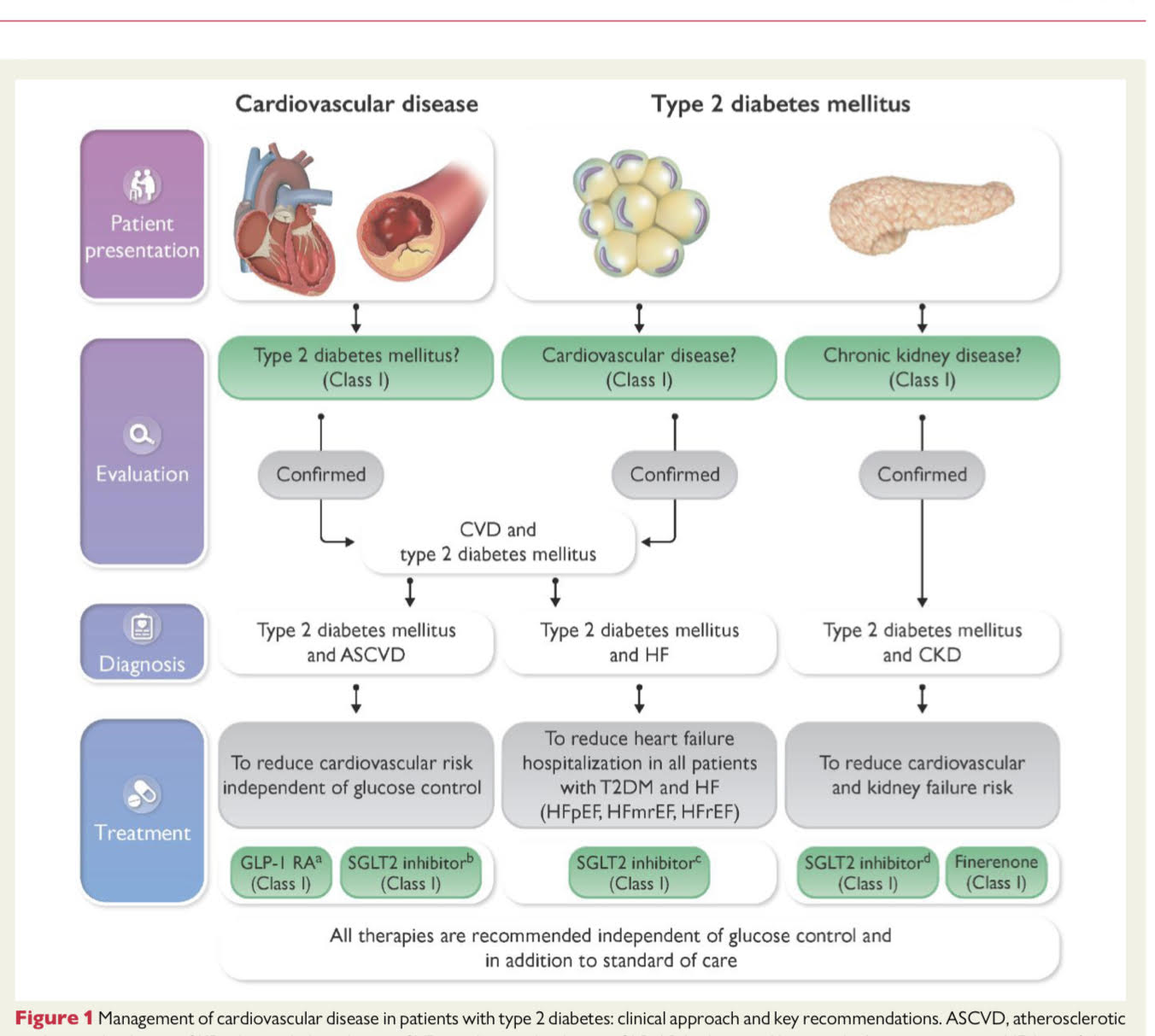
8. To reduce CV risk in patients with T2DM and ACSVD, it is recommended to treat with a GLP-1 receptor agonist and an SGLT 2 in- hibitor with proven benefit, on top of standard of care and independent of glucose control or target HbA1C.
9. In patients with HF—irrespective of ejection fraction—it is recommended that patients with T2DM are treated with an SGLT 2 inhibitor on top of standard of care to reduce HF-related endpoints such as HF hospitalization or CV death.
10. Patients with T2DM and CKD should be treated with an SGLT 2 inhibitor and the non-steroidal mineralocorticoid receptor antagonist finerenone to reduce both CV and kidney failure risk. In addition, these patients should receive a statin-based regimen, treat- ment with Angiotensin-converting enzyme inhibitors (ACE-I) or Angiotensin-II receptor blocker, and appropriate blood pressure control (≤130/80 mmHg).